

"Caramel" is a 4 1/2 old, spayed female, Persian that presented to me for her annual wellness exam. The owner reported all was well with Caramel.
She was acquired from the breeder as a kitten and is indoors only. Her past history was non-remarkable except for chronic bilateral epiphora. Her diet was Hill's t/d.
Physical Exam:

Can I play? Let's start with ruleouts for a young Persian cat. Here are some questions? Body condition score? Painful kidneys? PU/PD? HIstory doesn't say. Fever?
Rule outs for age and breed:
What did I miss?
Someone chime in on that or work up?
Good rule outs, Elizabeth!
This kitty lives totally indoors, with one other cat in the home. She is FeLV/FIV negative. No known history of toxin or foreign body ingestion. The owner was totally surprised that any abnormality was found on physical examination.
So we have a long list of rule outs for bilateral renomegaly, and we have to start crossing some of them off the list.
How do we do that?
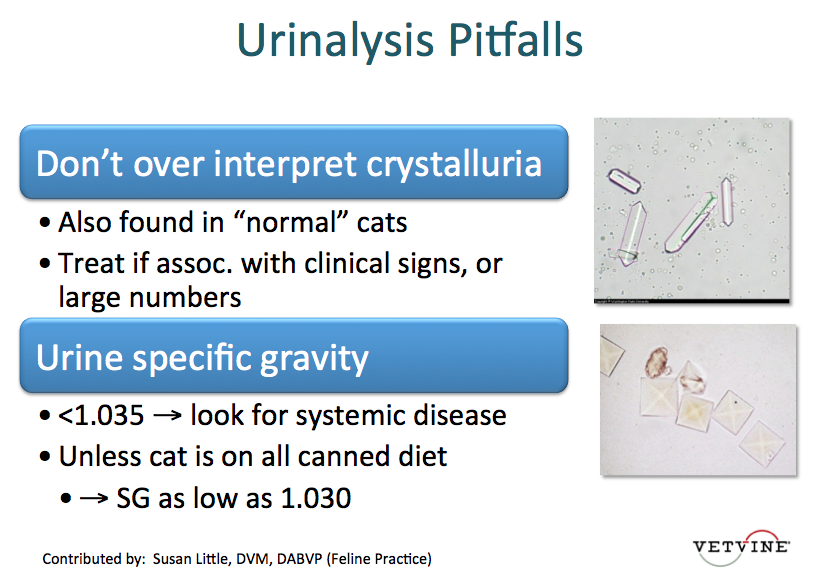
We started out by collecting a minimum database:
Thank you very much Dr. Little for this interesting case.
1. Specific gravity of the urine should not change with time.
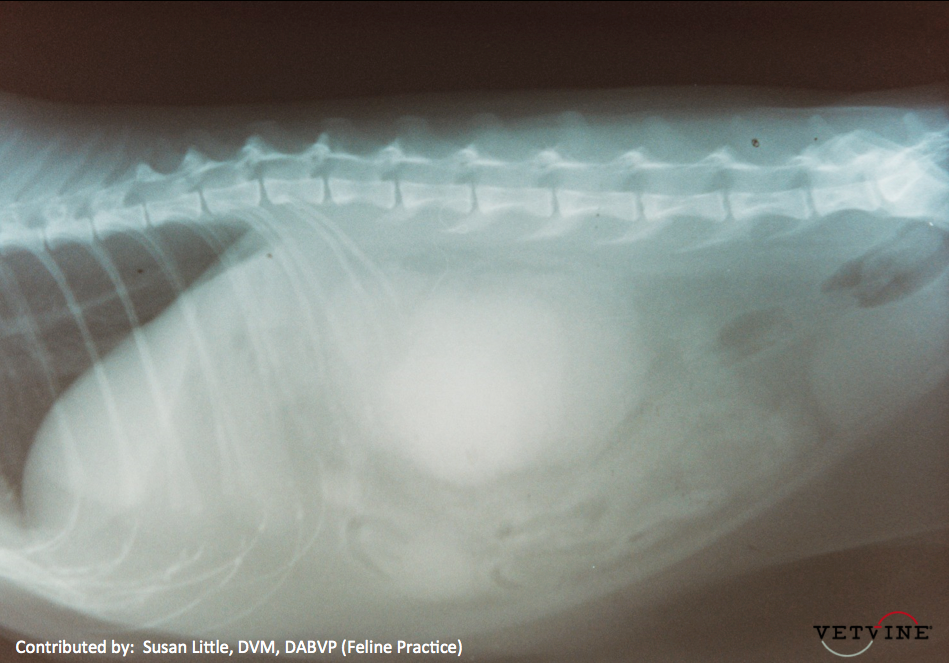
2. We see the VD radiographs and compare the size of kidneys to L2. ( In cats L is 2 to 3 times of L2, Width 3 to 3.5 cm.
3. To confirm the impession of bilateral renomegaly - VD radiograph is required.
4. 1. Lymphoma
2. Amyloidosis
3. Parasitic
4. Nephritis
Good thoughts Dr. Sood, though the kitty's indoor lifestyle might put parasites lower on the list. Another form of confirmation of bilateral renomegaly which might either change the differential list or confirm a diagnostic suspicion would be abdominal ultrasound.
Naturally, in the Persian breed one must include polycycstic kidney disease on the differential list. A few other causes are often not bilateral, such as pseudocyst, hydronephrosis, abscess or hematoma. Since this kitty has no symptomatic complaints, ethylene glycol is off the list as several symptoms pre-date renal effects.
Thanks Dr. Colleran.
Here is my confusion:
1. Polycystic kidney disease can be asymtomatic as in this case? In this disease should we feel the irregular kidneys?
2. If the client cannot afford the ultrasound, do you think urine Protein Cr ratio will help us as the sediment is quiet in this particular case?
3. Is there any indication for the kidney food at this stage?
Good questions, Dr. Sood. So sorry it took me a bit to get back to you. Quite often the cysts will just expand the size of the renal capsule, so the kidneys just look "big." They are sometimes irregular but not as often as "big."
Dr. Little reported that the sediment was quiet but not whether there was protein present in urine. If there were, I suspect she would have reported that as well. So UPC isn't going to say much. There is still good concentrating ability in this cat particularly if he eats both a moist and dry diet.
There is lots of controversy about renal diets and whether protein restriction or the attendant phosphorus restriction is really the benefit since those two characteristics have not been tested separately. In additon, the research done has only been for a duration of feeding of around 4 months. Our renal patients typically live a lot longer than that. There is a genetic test for Persian Autosomal Dominant Polycystic Kidney Disease that is done at University of California Davis and probably elsewhere by now. It doesn't tell you how seriously the cat is affected. It is intended to help diagnose early and remove cats from breeding programs.
Monday Mash-up:



That's interesting. Thank you all.
In this whole case, the only abnormal finding, so far - on physical exam - is the renomegaly. We are working on our refined list of differentials.
1. How to make the client undertsand to go ahead with this work up (Rads + ultrasound + biopsy) somewhere costs around $800 to $1000 when the client questions that the pet is doing well, why we are doing that? I apologize for this question but I face a lot of these clients who ask a lot of these questions. My second reason for this question is whenever we send the radiographs and patients for ultrasound, no specialist gives a straight forward answer, the reports are always in possibilities.
2. In our refined list of differentials, do the patients show any changes in the blood work or clinical symptoms, or do they remain asymptomatic until we do the ultrasound and find this out.
Thank you all.
We did proceed with an abdominal ultrasound for Caramel. For your reference, this is the appearance of a normal kidney on ultrasound:

Here are the images of Caramel's kidneys as viewed on abdominal ultrasound:


Abdominal ultrasound confirmed that Caramel has Polycystic Kidney Disease (PKD).
A little about PKD:
- This condition was identified in the 1960's in Persians and related breeds
- Some cats will go on to develop chronic renal disease, at an average of 7 years of age
This condition also occurs in humans:

Genetics and heritability play a role in this disease.

There is a PKD1 and Identity Marker test available that can indicate whether a cat has or will develop PKD (due to presence of PKD1 gene).
So ... regarding Caramel: what would be your plan and recommendations? Login and comment!

Regarding kidney size in cats, we found this in the Winn Feline Foundation Cat Health News:
Kidney Size in Three Cat Breeds:
Kidney disease is a common health concern in cats and ultrasonography is a useful tool for investigation and diagnosis of kidney disease. As a diagnostic imaging modality, ultrasound can offer important anatomical information such as kidney size, shape, and internal architecture. A change in kidney size, shape, and contour can be an indication of kidney disease. One area where changes in kidney size can be helpful is in the differentiation of acute kidney injury from chronic kidney disease. Increased size is more commonly seen with acute injury, whereas reduced kidney size suggests chronic disease.
In this study, kidney length, cortical thickness, medullary thickness, and corticomedullary ratio was determined in healthy cats belonging to three cat breeds: Sphynx (n =11), British Shorthair (n = 15), and Ragdoll (n = 15). Of all these measurements, renal length showed the highest variation among the breeds. Overall, individual and kidney side (right versus left) variation were more pronounced than the interbreed variation. Sphynx cats were inclined to have larger kidneys (4.09 ± 0.33 cm) than British Shorthair (3.77 ± 0.43 cm) and Ragdoll cats (3.87 ± 0.41 cm). However, British Shorthair cats were inclined to have a thinner renal cortex and medulla (0.67 ± 0.13 cm and 0.76 ± 0.18 cm respectively) than Sphynx (0.76 ± 0.14 cm and 0.90 ± 0.25 cm respectively) and Ragdoll cats (0.75 ± 0.13 cm and 0.91 ± 0.22 cm respectively). In the end, however, the tests did not reveal significant statistical differences between these particular cat
We continued to monitor renal function, blood pressure, and UPC at annual wellness exams and provided owner education regarding the condition and signs to look for that might indicate progression. It should noted that no drug or diet is known to change progression of this disease.
IRIS (International Renal Interest Society) has a schematic for staging chronic kidney disease in cats:

There is further substaging of the disease based on UP/C and systolic blood pressure (for assessing risk of end organ damage from hypertension):

Cats with chronic renal disease can develop hypertension, proteinuria and elevations in phosphorus, as well as other changes (below). Management strategies to consider include:
Share any other therapies you incorporate into the care of your patients. Did I miss anything? Login and comment.
I wanted to share the rest of this case - demonstrate the slow progression of Caramel's disease:
Iniitial diagnosis: November 2001 - IRIS Stage 2
Annual Wellness Exam: March 2005 - Stable / IRIS Stage 2
Annual Wellness Exam: May 2007 - Occasional vomiting was reported; 3% weight loss - IRIS Stage 2
Annual Wellnees Exam: August 2009 - Owner reported PU/PD, irregular appetite, 18% weight loss, BCS 3/9 - IRIS Stage 3
July 2010 - Euthanized
This is what her blood work looked like at each point:
In 2009, we made some adjustments to her care (she had progressed to Stage 3):
