
Forums
Guidance, support and wisdom to benefit and maximize the life and longevity of animals.
with a password reset link.
Be sure to check your SPAM folder if it's not in your inbox
Can't find it?
Need Help? Contact Us
Guidance, support and wisdom to benefit and maximize the life and longevity of animals.

VetVine Client Care
Chocolate consumption and associated toxicity is a problem that commonly results in a medical emergency. Peak times of exposure occur during "Chocolate "Season" - Halloween, the Christmas / winter holidays, Valentine’s Day, and Easter.
Chocolate is made from cocoa which contains methylxanthines (alkaloids). These compounds form naturally in plants and are also found in tea, coffee beans, cocoa beans and kola nuts. The toxic effects of chocolate in dogs are due to the presence of two alkaloids - theobromine and, to a lesser extent, caffeine.
Methylxanthines act by blocking adenosine receptors; Adenosine is a bronchoconstrictor, anticonvulsant, and regulates normal heart rhythm. The effects of toxicity are manifested by an overstimulation of the central nervous system (CNS) and cardiovascular system.
Clinical signs usually develop within 6-12 hours of ingestion and can include polydipsia (increased water consumption), vomiting, diarrhea, bloating, restlessness and hyperactivity - which can progress to ataxia (wobbly gait), tremors and seizures, cardiac effects (PVCs, tachycardia / increased heart rate), tachypnea (rapid breathing), hypertension, hyperthermia and coma. Pancreatitis is another possible consequence of chocolate ingestion as it has a high fat and sugar content and may contain nuts.
In dogs, clinical signs are expected with the following amount of methylxanthine consumption:
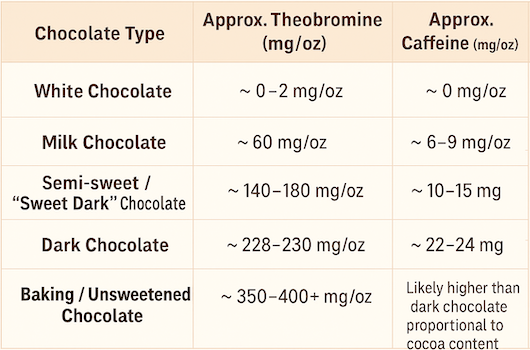
The levels of theobromine and caffeine vary between different types of chocolate. Typically, the darker the chocolate, the higher the cocoa and theobromine content.
Calculating the dosage of methylxanthine exposure is an important step in managing these cases. It is often difficult to identify the amount and type of chocolate used in products from a bakery or a pre-packaged mix, chocolate-filled candies and chocolate-covered nuts. Therefore, it is best to assume the worst-case scenario and calculate the dosage as if the product was solid chocolate.
First, determine the amount of methylxanthines in the type of chocolate ingested (using the information above), and then calculate the dosage of total methylxanthines per kg of patient body weight.
As an example:
A 9 kilogram (~20 lbs) dog eats 5 oz dark chocolate. Sweet dark chocolate (40-60% cocoa) contains approximately 150 mg theobromine and 10 mg caffeine per ounce. To calculate the dose of total methylxanthines consumed:
5 oz X 160 mg/oz = 800 mg and 800 mg divided by 9 kg equals 88.9 mg/kg as the total methylxanthine exposure in the dog.
Calculating the dosage for gourmet chocolate bars containing chocolate liquor is a little different. Chocolate liquor is cooled into blocks and is often used as unsweetened baking chocolate. The % cocoa actually refers to the % of chocolate liquor in the bar. To calculate the dosage in those cases, the % cocoa listed on the label should be multiplied by the value for unsweetened baking chocolate (~400 mg/oz). Therefore, a 70% bar would have (0.7 X 400) = 280 mg/oz and a 9 kg dog would only have to eat 2 oz to develop toxicity (~60 mg/kg).
Management of chocolate exposure includes stabilizing the patient then deciding on decontamination options.
Monitoring of the patient should include heart rate and rhythm, blood gases, and pancreatic enzymes. Supportive care for hospitalized patients may include thermoregulation, diazepam, barbiturate, methocarbamol for tremors / seizures, and oxygen as needed for cardiopulmonary compromise. Cardiac arrhythmias, if present, are treated with propranolol / esmolol. Intravenous fluids are administered to enhance excretion and provide cardiovascular support. A urinary catheter can be placed to decrease the reabsorption across the bladder wall or, alternatively, the patient should be walked frequently to encourage urination.